I got my last blood test results back and stared at the cholesterol section for a good ten minutes, trying to work out whether I should be worried. It was beyond confusing, and I didn’t really understand what I was looking at. Plus, as my dad always had high cholesterol during his life, it’s something I take seriously and want to understand.
There was a total number, a smaller number next to HDL, a bigger one next to LDL, something called triglycerides, and a ratio. The nurse said it all looked fine. The internet, when I got home and made the mistake of typing my numbers in, said I was either about to keel over or doing brilliantly, depending on which site loaded first. Note to self, never self-diagnose if you want to sleep well at night.
If you’ve had a cholesterol test recently, you’ve probably had the same experience. A row of numbers, a vague thumbs-up or a furrowed brow from whoever read them out, and absolutely no real sense of what any of it means for your actual life.
What Your Cholesterol Numbers Actually Mean
Your results sheet usually shows four things: total cholesterol, HDL, LDL, and triglycerides. Total cholesterol is the one most people fixate on because it’s the biggest number, and it sits at the top. It’s also the one that tells you the least on its own. It’s a sum of the others, and a sum can hide a lot.
HDL is the one people call the good kind. It’s a carrier that scoops up cholesterol from around the body and takes it back to the liver to be processed out. Higher HDL is generally a good sign for heart health, and most labs flag anything under about 40 mg/dL in men or 50 mg/dL in women as low.
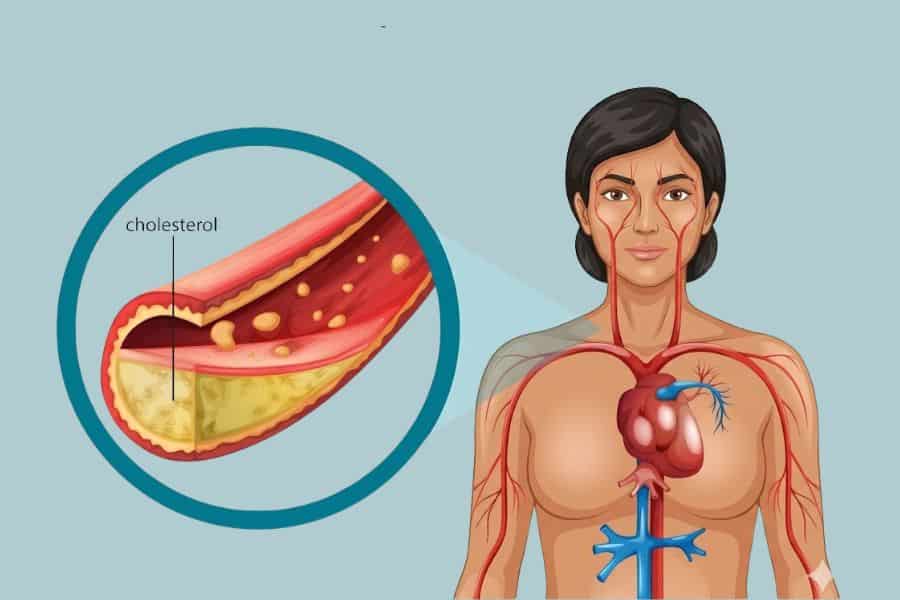
LDL is the one labeled “bad” because it carries cholesterol into the bloodstream, where, under the wrong conditions, it can build up in artery walls. Lower LDL is usually what doctors are aiming for, and the targets shift depending on whether you’ve had heart trouble before or have other risk factors.
Triglycerides are a different thing again. They’re a type of fat your body makes from excess calories, particularly from sugar, refined carbs, and alcohol. When you eat more than you burn, your liver turns the extra into triglycerides and stores them.
High triglycerides often travel with low HDL, and that combination is a bigger red flag than a high total cholesterol number on its own. There’s a good piece of research on this that’s worth a look if you want the proper detail, and you can read the study on triglyceride-to-HDL ratios and cardiovascular risk.

Why The Total Number Is Almost Useless On Its Own
Imagine two people with identical total cholesterol of 220. One has high HDL, low LDL, and low triglycerides. The other has rock-bottom HDL, high LDL, and triglycerides through the roof. Same total, but wildly different risk profiles. One is probably fine, while the other needs some thought.
This is why I get a bit twitchy when someone proudly tells me their cholesterol is 180 or 200, as if a single number settles it. It doesn’t. The ratios matter more. The two that doctors actually pay attention to are total cholesterol divided by HDL and triglycerides divided by HDL. Lower is better on both.
If your HDL is robust and your triglycerides are sensible, a total number that looks a bit high often isn’t the alarm it appears to be on paper, so breathe easily.
There’s also a particle called Lp(a), which most standard tests don’t include unless you ask. It’s largely genetic, meaning lifestyle changes won’t shift it much, and high levels independently raise heart disease risk.
If heart trouble runs in your family, as it does in mine, as my dad died of a heart attack, and your usual numbers look normal, this is the one worth asking about. I had to specifically request mine, and even then, the GP raised his eyebrows. I then tried to explain, in my broken French, why I wanted to know. It’s about the only time I wish I lived in an English-speaking country.
What The Evidence Actually Says About Food
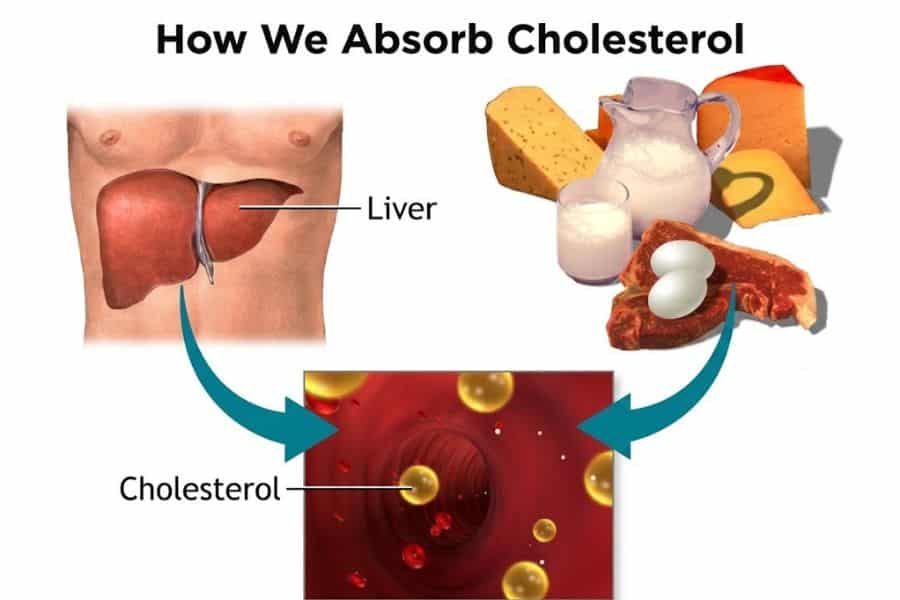
For decades, we were told dietary cholesterol was the villain. Eggs were public enemy number one. Then the advice shifted, and now most guidelines say the cholesterol you eat has only a modest effect on the cholesterol in your blood for most people.
Saturated fat got the next slot as chief villain, then refined carbs and sugar muscled in, and now it’s a bit of a free-for-all depending on which expert you follow on social media this week.
What the better-quality research keeps pointing to is less dramatic than any single food rule. Soluble fiber, the kind in oats, beans, lentils, apples, pears, and psyllium, lowers LDL because it binds to cholesterol in the gut and carries it out before it gets reabsorbed.
Unsaturated fats, particularly from olive oil, nuts, avocados, and oily fish, tend to improve the HDL-to-LDL picture when they replace saturated fat from processed meat and ultra-processed snacks.
I switched my afternoon cookie habit for a handful of almonds and a piece of fruit about two years ago, mostly because I was hungry by 4 pm anyway, and my next blood test showed my HDL had crept up and my triglycerides had dropped.
One person, one anecdote, take it for what it’s worth. But the food swap itself is backed up across a lot of trials. Cutting back on sugary drinks and alcohol does more for triglycerides than almost any other single change.

Movement, Weight, And The Boring Stuff That Actually Works
Exercise raises HDL and lowers triglycerides more reliably than almost any food tweak. Brisk walking, cycling, swimming, anything that gets you a bit puffed for about 150 minutes a week, is the threshold most of the research lands on.
Resistance training a couple of times a week helps, too, mostly because muscle is metabolically active and changes how your body handles fats and sugars over time.
Losing even a small amount of weight if you’re carrying extra around the middle has an outsized effect on triglycerides and HDL. Not the whole-body weight loss the magazines push, but a 5 to 10 percent drop tends to shift the numbers meaningfully.
The middle matters more than the scale does, because visceral fat (the kind that wraps around your organs) is the type that messes with how your liver processes fat.
Sleep and stress are the two everyone wants to skip because they’re harder to fix than swapping butter for olive oil. Chronic short sleep and chronic stress both nudge cholesterol numbers in the wrong direction, partly through cortisol and partly through their effects on appetite and food choices.
I’m not going to pretend I’ve cracked either of those. I’m still wearing the eye mask and still occasionally giving up and doom-scrolling at midnight. But the nights I do sleep properly, my eating the next day is dramatically less chaotic, and over months, that’s the kind of thing that shows up in bloodwork.
What To Ask At Your Next Appointment
If you’re going in for results or asking for a test, a few specific questions will get you more useful information. None of this is medical advice; it’s just what I wish I’d known to stop all the fruitless Googling.
Questions to ask
- What’s my LDL on its own, and what’s my HDL? The total number alone isn’t enough to act on, and most GPs will happily walk you through the breakdown if you ask.
- What’s my triglyceride-to-HDL ratio? This one rarely gets mentioned out loud, but it’s a more honest snapshot of metabolic health than total cholesterol.
- Should I have an LP (a) test, given my family history? Worth asking once in your life, because it’s largely genetic and a one-off test gives you information you’ll have forever.
- Are there any non-cholesterol markers worth checking? Things like fasting glucose, HbA1c, and high-sensitivity CRP round out the picture, and most labs run them on the same blood draw.
- If my numbers are off, what would you like me to try first before we talk about medication? A good GP will be happy to give you three to six months of food and movement changes before reaching for the prescription pad, unless your risk is high enough that waiting isn’t sensible.
The one thing I’d add, and this is from sitting in a few of these appointments myself, is that you’re allowed to ask for the actual numbers rather than a verbal summary. Get a copy. Look at them yourself. Track them over a year or two.
A single test is a snapshot, and snapshots sometimes lie. A pattern across three or four tests, with notes on what you were eating, how you were sleeping, and whether you’d just had a stressful month, is what actually tells you what’s going on with your heart.
Disclaimer: This article is for general information only and isn’t a substitute for personal medical advice. If you have concerns about your cholesterol or heart health, talk to your GP or a qualified healthcare professional who can look at your full history.